The Substance Abuse and Mental Health Services Administration (SAMHA) recently issued a report based on new survey results. One area of focus was major depression among adolescents.
Service Utilization Among Depressed Adolescents
Major findings from the survey included the following:
- 1.9 million youth (8% of the population) between the ages 12-17 experienced a major depressive episode in 2010, a rate in line with recent years and slightly less than rates of around 9% in 2004. The rate increased with age from 3.3% among 12 year olds and 10.9% among 16 year olds.
- Major depression was more common in females (11.8% versus 4.4%)
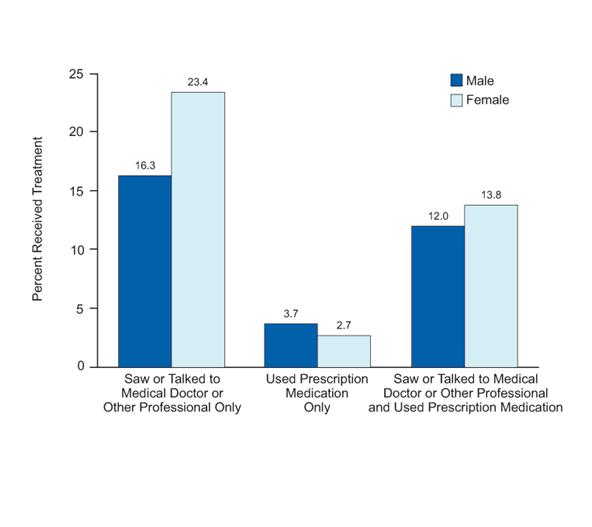
- Only 37.8% of youth with depression sought out a professional (defined as seeing or talking to a doctor or other professional)
- 16.3% of depressed youth were treated with medications (with or without other types of treatment), while the remaining 21.4% saw or spoke to a doctor or other professional without using medication
- Only 3% of depressed youth were treated with medications only without seeing a medical or mental health professional
While the accuracy of survey data can be questioned, the rate of 8% found here is actually below the rate of 11% found in a more rigorously diagnosed group in the National Comorbidity Study of Adolescents.
These data cannot be used to examine the question of whether teens who are not depressed are receiving diagnoses and treatment inappropriately. Nonetheless, the results do suggest that most depressed adolescents, even those with significant impairment, are receiving no treatment at all of any kind.
Questions related to the overdiagnosis of mental illness and overuse of medications are important ones, but we shouldn’t lose sight of findings like these that indicate that most depressed teens who need our help are not getting it.
The report can be found at http://www.samhsa.gov/data/NSDUH/2k10MH_Findings/2k10MHResults.htm